Brain Pacemakers in Consumer Medical Electronics Improve Quality of Life
Citation: K. Michael, "Brain Pacemakers in Consumer Medical Electronics Improve Quality of Life: Benefits, Risks, and Challenges," in IEEE Consumer Electronics Magazine, vol. 7, no. 4, pp. 82-85, July 2018, doi: 10.1109/MCE.2018.2816298.
{kind=link}
I recently (8 September 2017) had the pleasure of speaking with Gary Olhoeft, who, in 2009, had a deep-brain stimulation (DBS) device implanted to help him combat Parkinson’s disease. Dr. Olhoeft is a retired emeritus professor of geophysics at the Colorado School of Mines, Golden. He previously taught a number of subjects related to advanced electrical and electromagnetic methods, antennas, near-surface field methods, ground-penetrating radar, and complex resistivity.
This interview is a participant observer’s firsthand journey into a life dependent on a deep-brain stimulator. Of particular interest is the participant’s qualifications in the field of electromagnetics with respect to his direct experience of the benefits, risks, and challenges surrounding the device that has been implanted in his body. I first came to know of Dr. Olhoeft’s work while exploring the risks associated with biomedical devices in general, through his open comments in a Gizmodo article in 2017 [1]. Dr. Olhoeft has also delivered numerous presentations to the EMR Policy Institute on “Electromagnetic Interference and Medical Implants,” dating back to 2009 [2].
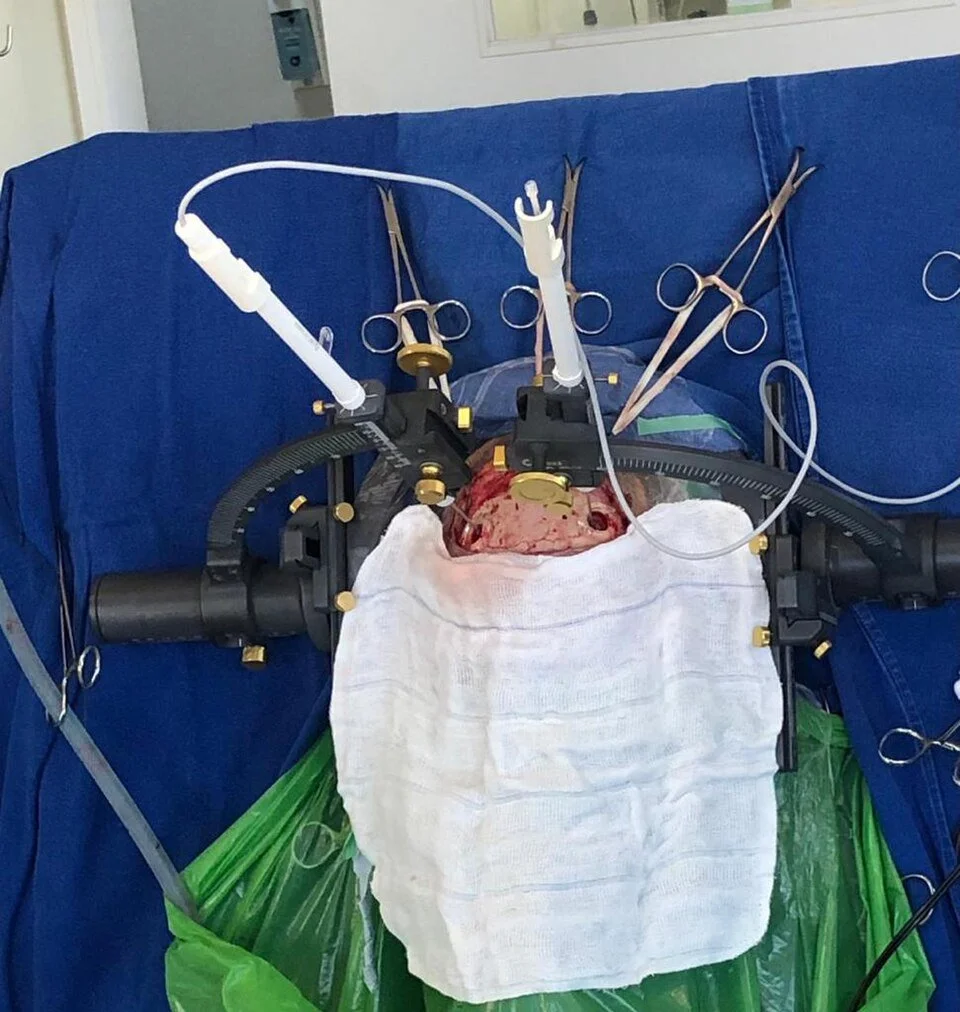
Katina Michael: Gary, as more people come on board with various brain implants, heart pacemakers, and internal diagnostic devices, I think that the U.S. Federal Communications Commission [FCC], the U.S. Food and Drug Administration [FDA], and the health insurance industry more generally will have to engage with at least some of the issues that you and other biomedical device recipients have identified from your experience. So many people who are designing biomedical devices do not actually realize that patients are awake during some of the DBS procedure. I found, on the engineering side of the design, that many engineers have never witnessed a DBS going into someone’s brain or at least understood the actual process of implantation. I do find it bewildering that some engineers have never spoken to patients or are so withdrawn from the practical side of biomedical device deployment. Engineers tasked with some complex problems sometimes look at only solving a single part of the end-to-end design without understanding how all the componentry works together.
Gary Olhoeft: I was also amazed to talk to the chief engineer at Medtronic about the DBS once. He told me the whole thing was entirely built out of discrete components with no integrated circuits because the FDA has not approved any integrated circuits yet.
Michael: What do you make of this—that the regulations and the regulatory body responsible are holding things up? What is your personal position?
Olhoeft: Well, I definitely think that the regulatory body is holding things up. Just look at when the first DBS was installed in France in 1987. It was something like 14 years before it was made available in the United States, in about 2001, with FDA approval. I got mine in 2009, and they had already sold hundreds of them at that point in America.
Michael: And for you at that time, there was no other alternative? I assume that if you had not adopted, that your quality of life was going to diminish quickly?
Olhoeft: That’s right. I would have continued shaking and not been able to write, or I would have avoided reading or walking or talking. Something I think I haven’t told you yet is that my device is also an interleaved device that has two settings that alternate; one is set for me to walk, and the other is set for me to talk. You used to have to choose between the two, but now they can alternate because they are interleaved, so that I can do both at the same time.
Michael: For me, Gary, it is nothing short of a miracle what these biomedical engineers are doing. Was the FDA correct in waiting those 15 years or so before they gave their approval, or they should have approved earlier so other people might have had an improved quality of life in the United States?
Olhoeft: It depends on what they are talking about. Some of the things they are talking about with genetic modification implants—with viral-inducing genetic modifications and stem cells—these things are going too fast. A doctor once told me, when they go to the FDA for approval, they have to go through trials. The first trial involves a few people. The next involves a few tens of people. And then, at the approval point, there are hundreds of people. But then, when it is approved, possibly hundreds or thousands or millions of people will get it, and next all kinds of things can go wrong that they did not anticipate. So you have to be very careful about this stuff. However, the FDA seems to reinvent the wheel, requiring their own testing when adequate testing has already been done in other countries.
Of particular interest is the participant’s qualifications in the field of electromagnetics with respect to his direct experience of the benefits, risks, and challenges surrounding the device that has been implanted in his body.
Michael: I agree with you. It is the brain we are talking about after all.
Olhoeft: The thing that bothers me most is that Apple footage you sent me [https://www.youtube.com/watch?v= h6cIeZmFdPs]. You know, that clip with Steve Jobs and the Wi-Fi problem? I would not have liked to have been in that room with a DBS.
Michael: Yes. And, if he could not run an iPhone demo with that EMC [electromagnetic compatibility] interference problem when we know Jobs would do exhaustive user testing at launches, then what are we going to do, Gary, when we have more and more people getting implants and even more potential electromagnetic interference? I am trying to figure out what kind of design solution could tackle this.
Olhoeft: And there’s a whole bunch of other things that bother me, like the electromagnetic pulse to stop cars on freeways and the devices they have to shock people. What about all those people who have implants like me or other kinds of implants? In one of those fictitious mystery shows, someone was depicted as being killed in a bank robbery, and he was killed by an electromagnetic pulse. So we can see these kinds of scenarios are making it into the public eye through the visual press.
Michael: And that was a fictional account, right?
Olhoeft: It was a fictional scenario, but it is certainly possible. Do an Internet search on “nonlethal electric shock devices” like stun guns, and you’ll find people have been killed by them. In Arizona, last month, a woman was run over and killed by an Uber in autonomous mode. Earlier in the year, a Tesla in autonomous mode killed its driver.
It is really about the importance of including the end user, or patient in this case, in the product life cycle management process.
Michael: Yes, it sure is. Exactly. I am speaking at the annual conference for the Australian Communications Media Authority next month, and I will be using our discussion today as a single case study to raise awareness. Presently, some biohackers are even talking about hacking the brain, and I am telling them you really should not be doing that without medical expertise, even if it is in the name of citizen science. Some of them are amateur engineers, and others are fully fledged, qualified engineers but not medical people. And I personally feel the brain is not to be experimented with like this.
Olhoeft: It is like DARPA. They have a call-up at the moment to have a million electrodes inside the brain so they can communicate, not for therapeutic value like I have [3].
Michael: You are likely familiar with the DARPA project from 2012 for a brain-implantable device that could be used to aid former servicemen and -women suffering from posttraumatic stress disorder, depression, and anxiety [4]. We did a special issue on this in IEEE Technology and Society Magazine last year [5]. They have also claimed this device solution could be used for memory enhancement. It sounds like the cyborgization of our forces.
Olhoeft: That’s like what I have. The latest one is more like when you want to remote-control a vehicle or something. The September 2017 IEEE Spectrum had an article about Brain Racers using brain-controlled avatars to compete in a cyborg Olympics [6].
Michael: And the communications for autonomous weapons or override. Can a human be autonomous, for instance? Last week, we were discussing some of the ethics behind overriding someone’s decision not to fire or strike at a target. Or imagine the ability to remotely control a drone just by using your thoughts, versus someone in a remote location executing the fire or strike commands without being in situ, by intercepting that communication stream. Imagine the potential to intercept a person’s thoughts and to make them physically do something. This is where, for me, the waters get muddied. I do not mind the advancements in the cochlear space for instance, where deaf persons have the ability to hear music and entertainment through an embedded technological device. I think that is another marvel, really. But I’d be interested to hear your opinion about the crossover between the medical and nonmedical spaces. Do you think that is just life? That is just how innovation is? That we need to get used to this? Or do you believe prosthetics are the only reason we should be implanting people in the brain?
Olhoeft: I think the only reason we should be implanting people is for therapeutic reasons. For instance, I have a deep-brain stimulator for a specific disease. Others might have a particular problem, or maybe it is to replace a part of the brain that has been damaged physically. Because the question becomes, [do] we [become] no longer human if we go beyond prosthetics purposes? We have problems with driverless cars, for instance, and people are talking about mirrored systems and all sorts of electronics in them that interfere with DBS. There was a paper that was published where researchers took about ten cars at different times, and they discovered that the ones that were diesel powered did not interfere, because they didn’t have any ignition system [7]. Conventionally powered cars that had an electronic ignition system pad caused some interference. But electrics and hybrid engines had problems with people with implants [8]–[10].
Michael: So do you fear getting in a vehicle at any time?
Olhoeft: A Prius has eight computers inside it, Wi-Fi, and Bluetooth, and the way they run the wiring from the batteries to the front, it is not twisted wiring, it is just a straight pair of wiring. If it was a twisted pair, there would be a lot less magnetic noise inside the car body.
Michael: So that’s the car company trying to save money, right?
Olhoeft: I really don’t know. We have a Prius as well. I’ve tested our car. We have two sets of batteries. The front-right and rear passenger seats are okay, but the driver’s position is very noisy. There’s a woman we know, when she drives her Prius, her deep-brain stimulator turns off when the car goes into charging mode [while braking].
Michael: Oh dear, this is a major problem. These issues must get more visibility. They can no longer be ignored. This is where consumer electronics come head-to-head with biomedical devices.
Olhoeft: That’s why I don’t drive. I’ve also sent letters to the FCC and FDA, and I’ve not received any response.
Michael: This is truly an important research area. This topic crosses over engineering, policy, and society. It is really about the importance of including the end user, or patient in this case, in the product life cycle management process.
Olhoeft: Agreed.
Michael: I worry about potential hackers, predatory hackers, switching people off, so to speak, in the future. My concern is that the more of us who bear these implantables for nonmedical reasons in the future, the greater the risks.
Olhoeft: There is a well-known story of someone who has had an internal insulin pump hacked, and an insulin dose was changed so that it killed them [11], [12].
Michael: I do wonder, Gary, if this all has to do with liability issues. There is simply no reason that companies like Medtronic should not be engaging the public on these matters. In fact, it is in their best interest to receive customer feedback.
Olhoeft: It’s definitely a problem, and I don’t know what to do about that.
References
1. K. V. Brown. ( 2017, Mar. 7 ). Why people with brain implants are afraid to go through automatic doors. Gizmodo. [Online]. Available: http://www.gizmodo.com.au/2017/07/why-people-with-brain-implants-are-afraid-to-go-through-automatic-doors/
2. G. Olhoeft. ( 2009, Dec. 7 ). Electromagnetic interference and medical implants. The EMR Policy Institute. [Online]. Available: https://youtu.be/jo-B6LWfVzw
3. E. Waltz. ( 2017, Apr. 26 ). DARPA to use electrical stimulation to enhance military training. IEEE Spectrum. [Online]. Available: https://spectrum.ieee.org/the-human-os/biomedical/devices/darpa-to-use-electrical-stimulation-to-improve-military-training
4. R. A. Miranda, W. D. Casebeer, A. M. Hein, J. W. Judy, E. P. Krotkov, T. L. Laabs, J. E. Manzo, K. G. Pankratz, G. A. Pratt, J. C. Sanchez, D. J. Weber, T. L. Wheeler, and G. S. F. Ling. ( 2015, Apr. ). DARPA-funded efforts in the development of novel brain–computer interface technologies. J. Neurosci. Methods. [Online]. 244, pp. 52–67. Available: http://www.sciencedirect.com/science/article/pii/S0165027014002702
5. K. Michael, M. G. Michael, J. C. Galliot, and R. Nicholls. ( 2017, Mar. ). Socio-ethical implications of implantable technologies in the military sector. IEEE Technol. Soc. Mag. [Online]. 36 ( 1 ), pp. 7–9. Available: http://ieeexplore.ieee.org/stamp/stamp.jsp?arnumber=7879457
6. S. Perdikis, L. Tonin, and J. d R. Millan. ( 2017, Sept. ). Brain racers. IEEE Spectr. [Online]. 54 ( 9 ), pp. 44–51. Available: http://www.ieeeexplore.ws/stamp/stamp.jsp?tp=&arnumber=8012239&isnumber=8012214
7. R. Hareuveny, M. Sudan, M. N. Halgamuge, Y. Yaffe, Y. Tzabari, D. Namir, and L. Kheifets, “Characterization of extremely low frequency magnetic fields from diesel, gasoline hybrid cars under controlled conditions,” Int. J. Environ. Res. Public Health, vol. 12, no. 2, pp. 1651–1666, 2015.
8. N. Lou, ( 2017, Jan. 27 ). Everyday exposure to EM fields can disrupt pacemakers. MedPage Today/CRTonline.org. [Online]. Available: https://www.medpagetoday.com/cardiology/arrhythmias/63433
9. O. S. Pantchenko, S. J. Seidman, and J. W. Guag. ( 2011 ). Analysis of induced electrical currents from magnetic field coupling inside implantable neurostimulator leads. BioMed. Eng. OnLine. [Online]. 10 ( 94 ). doi: 10.1186/1475-925X-10-94. Available: https://biomedical-engineering-online.biomedcentral.com/articles/10.1186/1475-925X-10-94
10. K. Dustin. ( 2008 ). Evaluation of electromagnetic incompatability concerns for deep brain stimulators. Disclosures: J. Neurosci. Nurs. [Online]. 40 ( 5 ), pp. 299–303. Available: http://www.medscape.com/viewarticle/582572
11. D. Goodin. ( 2011, Oct. 27 ). Insulin pump hack delivers fatal dosage over the air. The Register. [Online]. Available: https://www.theregister.co.uk/2011/10/27/fatal_insulin_pump_attack/
12. BBC Staff. ( 2016, Oct. 4 ). Johnson & Johnson says insulin pump “could be hacked.” BBC News. [Online]. Available: http://www.bbc.com/news/business-37551633#
Authors
University of Wollongong, Australia
Katina Michael (katina@uow.edu.au) is a professor at the University of Wollongong, Australia, who has been researching the social implications of implantable devices for the last 20 years.
Citation: K. Michael, "Brain Pacemakers in Consumer Medical Electronics Improve Quality of Life: Benefits, Risks, and Challenges," in IEEE Consumer Electronics Magazine, vol. 7, no. 4, pp. 82-85, July 2018, doi: 10.1109/MCE.2018.2816298.