Brain Pacemakers in Consumer Medical Electronics Improve Quality of Life-Part II
Citation: K. Michael, "Brain Pacemakers in Consumer Medical Electronics Improve Quality of Life-Part II: The Need for Patient Feedback in the Product Lifecycle Management," in IEEE Consumer Electronics Magazine, vol. 7, no. 6, pp. 51-54, Nov. 2018, doi: 10.1109/MCE.2018.2835879.
The following is a continuation of the interview “Brain Pacemakers in Consumer Medical Electronics Improve Quality of Life,” published in the July 2018 issue of IEEE Consumer Electronics Magazine. It spotlights Gary Olhoeft, who, in 2009, had a deep-brain stimulation (DBS) device implanted to help him combat Parkinson’s disease. Dr. Olhoeft is a retired emeritus professor of geophysics at the Colorado School of Mines, Golden. He previously taught a number of subjects related to advanced electrical and electromagnetic methods, antennas, near-surface field methods, ground-penetrating radar, and complex resistivity.
{kind=link}
Katina Michael: In part one of this interview, we discussed electromagnetic interference with respect to brain pacemakers. So we need some hardcore evidence that someone’s implantable has previously been tampered with?
Gary Olhoeft: I’ve already raised the issue several times, and Medtronic, my brain implant manufacturer, just sent me the programmer’s manual for the patient. The original one I got was just a couple of pages and had to do with interference. The latest version is 16–18 pages in length on interference, and that is because of the questions I raised about interference and the evidence I showed them. They still won’t admit that their device was defective in one case where I could prove it. My doctor believed me because I showed him the evidence, so he had them replace it at no charge.
Michael: Is your DBS data uploaded through some mechanism, like the heart pacemaker data are uploaded on a nightly basis and sent back to base [1]?
Olhoeft: No, when I visit the doctor’s office is the only time they have access to it. Only when I go to the doctor.
Michael: You mean to download information or to check its operation?
Olhoeft: To download information from the pack in my chest. Actually, they store it in there. They print it out in hardcopy because they are afraid of people hacking their computers. And this is the University of Colorado Hospital.
Michael: Yes, I totally understand this from my background reading. I’ve seen similar evidence where hardcopies are provided to the patient but a lot of the patients, like Hugo Campos, are saying hardcopies are not enough. I should be able to have access at any time, and I should be able to tell someone my device is acting up or that something is wrong.
Olhoeft: Right. Remember how I told you about the interleave function? Well, when they set it to the interleave setting for the first time, they didn’t do it right, and I woke up the next morning feeling like I had had 40 cups of coffee. It turns out, it was running at twice the frequency it should have been, and I could show that. I called them up and said, “You’ve got a problem here,” and they fixed it right away. I figured I could measure it independently of the Medtronic device. That’s why I built my own ac wirewound ferrite core magnetometer to monitor my own DBS. But all the doctor had was a program that told him whatever Medtronic wanted to tell him. I wanted more information than that. I wanted to actually see it, so I built my own.
Michael: I saw your information that you would have had a product out on the market to help others, but the iPhone keeps upgrading.
Olhoeft: It keeps changing faster than I can keep up with it.
Michael: I am going to argue that it is their responsibility, the manufacturer’s responsibility, to provide this capability.
Olhoeft: I see no reason why they couldn’t, but I like the idea of a third party providing an independent measurement of whether the implant is working and measuring the parameters directly (i.e., pulse height, pulsewidth, pulse repetition frequency, and so on).
Michael: I am concerned on a number of fronts, and have been for some time. This is not particularly a huge ask if manufacturers are cooperative in the process of incremental innovation. For example, imagine if Apple collaborated with Medtronic or the other providers from Stryker and so forth, like Cochlear have already collaborated with Apple. I think biomedical device manufacturers have to offer this as a service and in layman’s understanding for nonengineers. And it must be free and not cost the recipient anything. It is the only way to empower recipients of the pacemakers and for them to feel at ease without having to go for a visit to a medical specialist.
Olhoeft: I told you about the experience of walking into a Best Buy and having their automated inventory control system turn off my DBS?
Michael: Yes.
Olhoeft: I used my device to see what frequency it was operating at and then asked my doctor to change my DBS to a different frequency so that I could walk in and out of Best Buy. So the frequency range means the operator needs to have such things in mind. These inventory-control devices are built into walls in stores and malls, so you no longer know that they are even there or have any warning. But they are there.
Michael: I know, they are unobtrusive.
Olhoeft: So there needs to be warning signs or other things like that. They seem to begin appearing in hospitals and imaging centers where they say, “MRI in use, if you have a cardiac pacemaker or brain pacemaker device, do not enter this room.” But it is a rare thing still. I remember 20 years ago or so when they had signs warning about microwave ovens being used.
Michael: Yes, I remember that.
Olhoeft: It is like we need a more generic reason than that.
Michael: What is your feeling with respect to radio-frequency identification? Or the new payment systems using near-field communications? Are they affecting pacemakers? Or is it way too low in terms of emissions?
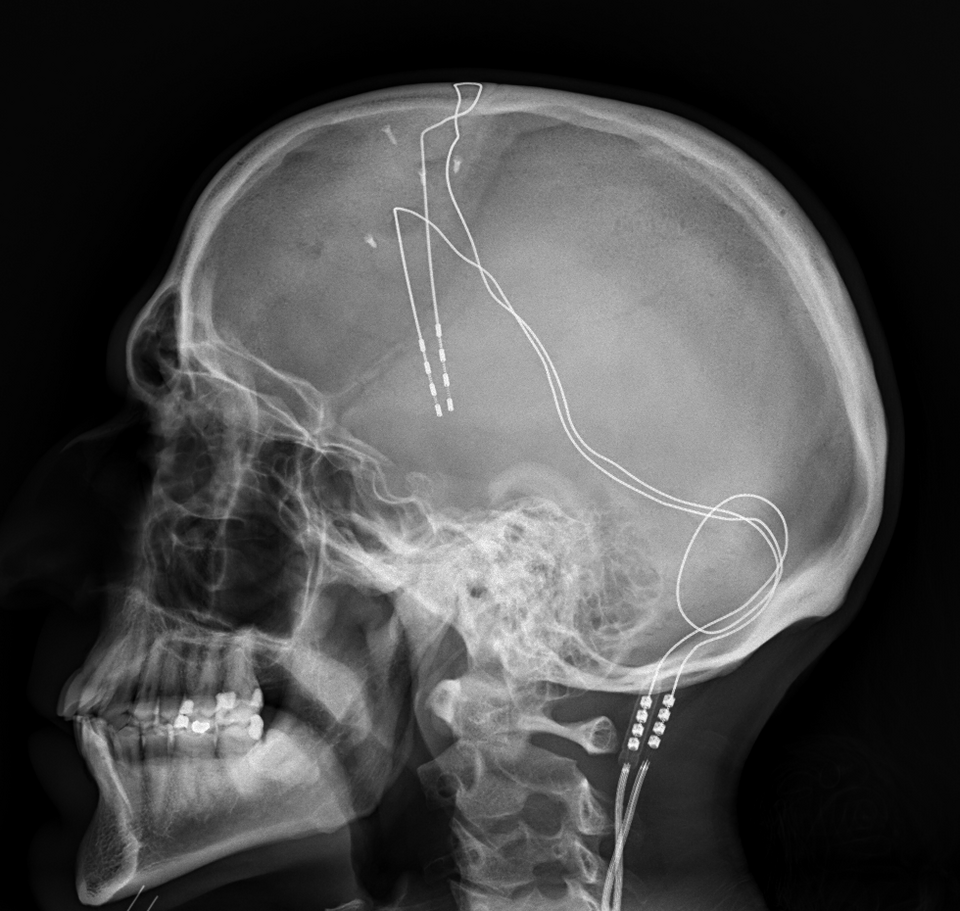
Olhoeft: Well, no. There are wireless devices that are low-level that don’t bother me. For example, I have a computer with Wi-Fi, and that doesn’t bother me. That is because I’ve measured it, and I know what it is. It is a dosage thing. If I stay near it, the dosage begins to build up, and, eventually, it can get to a point where it could be a problem. Not necessarily for my DBS but for other things. Heart pacemakers are much closer to the heart, so there is less of a problem, and the length of wiring is much shorter in heart pacemakers. I have a piece of wire that runs from my chest, up my neck, up over the top of my head, and back behind my eyes; it is almost 18 in long. That is part of the problem. They could have made that a twisted pair with shielding like CAT6 wiring, but they didn’t. The Medtronic people need to fix that one.
Michael: I spoke to some researchers in June last year who were talking about not having the battery packs so low, having them closer to the brain and smaller in size. Do you think the problem would dissipate somewhat if the battery pack was closer to the brain?
Olhoeft: Yes. But then the battery won’t last as long because it’s smaller. They are already trying rechargeable batteries, but you spend all day at the charger; you get 9 h of charging for only 1 h of use. So my doctor told me that, and he did not recommend that for me.
Michael: Do you find a conflict in your heart sometimes? You are trying to help the manufacturer make a better product and raise awareness of the important issues that patients face, and, yet, you are relying on the very product to which you are trying to get some response. Have you ever written to Medtronic and said, “This is my name, and this is my story, would you allow me to advise you, that is, provide feedback to your design team” [2]?
Olhoeft: There is a vice president who is responsible for research and development who is both a medical doctor and an engineer. I wrote to him several times and never got an answer, but I have spoken to Medtronic’s chief engineer about my device misbehaving, you know, with all those missing pulses. He was quite open about it. I also told him about the interleave problem at that time that it felt like I had had 40 cups of coffee, and he said that was outside his area of expertise because he built the hardware but someone else programmed it. There are books out there that might tell you how to program these things. I’ve looked at them, but I don’t agree with the approach they take. They never talk about interference. The default programming for this is 180 repetitions; it’s still the wrong place to start because, in the United States, 180 is a multiple (i.e., harmonic) of the powerline and close to the frequency used by many security systems and inventory-control systems.
Michael: I am so concerned about what I am hearing. Concerned that the company is not taking any action and that we are not teaching our up-and-coming engineers about these problems. As our medical devices increase in sophistication, engineers in training and practice must know how to avoid or overcome the known pitfalls. I am also concerned that recipients of these brain pacemakers are not given the opportunity to provide proper feedback to design teams directly, and that there is no indirect path in which to do this. A website does not cut it. There are people, like yourself, Gary, who are willing and have relevant research expertise, who these companies should be welcoming onto their payroll to improve the robustness of their technologies.
It is important to create a safe space where manufacturers, medical practitioners, patients, and policy makers come together to discuss these matters openly.
Olhoeft: Well, I’ve tried writing to various organizations and agencies and, when possible, giving testimony to the U.S. Food and Drug Administration (FDA), the U.S. Federal Communications Commission (FCC), and other agency requests for information. One of the problems seems to be that the technology is changing much faster than regulators can keep up with.
Michael: I think it is important to create a safe space where manufacturers, medical practitioners, patients, and policy makers come together to discuss these matters openly. I know there are user groups where patients go to discuss issues, but that serves quite a different function, as more of a support group. But until there is some level of openness, then it will be likely that these issues will continue to cloud future developments. Gary, we need more people like yourself who have real stories to share, that are documented, together with peer-reviewed published research in the domain of interference and DBS. We should continue to write to them and also invite them to workshops and roundtable meetings, invite representatives from the FDA and FCC. What do you think about this approach?
Olhoeft: Yes, you can put me down for that. I’ll be involved. Part of the problem is that the FCC authorization says 9 kHz up to 300 gHz. And these devices operate at below 200 Hz. So the FCC has no regulatory authority over them, except as Part 15 devices. The FDA has no limit. From lasers down to dc. The FCC has nothing to do with it, so we need to get involved with the FDA. We need them to get to document things at any rate.
Michael: The Internet of Things (IoT) is promising so much in the electronics market. I think the last statistic I read that the media caught wind of was 50 billion devices by 2020 [3].
Olhoeft: You are looking at a house that could have every lightbulb, every appliance, every device in it on the Internet.
Michael: Yes indeed, we just have to look at the advent of NEST.
Olhoeft: And, yet, they are wirelessly transmitting. It would be much better if they were hooked up using fiber optics.
Michael: Agreed. I mean, for me, it is also a privacy concern with everything hooked up in the house to the Internet [4]. Last year, somebody demonstrated they could set a toaster alight in an IoT scenario. At IEEE Sections Congress in 2017, I spoke to several young people involved with driverless cars. And, I don’t know, they were very much discounting the privacy and security issues that will arise. One delegate told me, “It’s all under control.” But I do not think they quite get it, Gary. I said to one of them, “But what about the security issues?” He replied, “What issues? We’ve got them all under control. I am not in the slightest concerned about this because we are going to have protocols.” And I pointed to the Jeep Cherokee case where some hackers got it to stop in its tracks on a highway in the United States [5]. One of my concerns with these driverless cars is that people will die, sizzling in a hot vehicle, where they have been accidentally locked inside by the “car.” And they don’t even have to have pacemakers; it is an issue of simply having a vehicle unlock its doors for a client to exit.
Until there is some level of openness, then it will be likely that these issues will continue to cloud future developments.
Olhoeft: There was the case of the hybrid vehicle that was successfully stopped and [it was] demonstrated on TV.
Michael: Yes. And there was also someone wearing an Emotiv device that was steering their vehicle with their thoughts [6]. What if I hacked into the driver’s thoughts during transmission and steered the car off a cliff?
Olhoeft: So what will they do between vehicles when the devices start to interfere with one another?
Michael: Yes, exactly! And when devices begin interfering with one another more frequently for who knows what reason?
Olhoeft: We have had situations in which cell phones have stopped working because the network is simply overloaded on highways or blocked by landslides or just traffic congestion. The Broncos football stadium here is undergoing a US$6 million upgrade just so they can get the Wi-Fi working, and now they are building it into every seat. They now have security systems like airports do, and so I cannot go into the stadium anymore because of my DBS. I couldn’t sit in a light rail train either.
Michael: So here is a more metaphysical and existential question. I am so fortunate to be speaking to you! You are alive, you are well in terms of being able to talk and communicate, and, yet, somehow, this sophisticated technology also means that you have had to dull down your accessibility to certain places, almost living off the grid to some degree. So, all of this complex technology actually means you are living more simply, perhaps. What does that feel like? It really is a paradox. You are being careful, testing your devices, testing the Wi-Fi, and learning by trial and error on the fly, it seems.
Olhoeft: Well, I have a landline phone against my head right now because I know it doesn’t bother me. I cannot hold a cellular phone within 20 in of my head. So you are right. I mean, there are a lot of places I cannot go to, like the school library or the public library because of their system for keeping track of books. It has a very powerful electromagnetic pulse. When I go to the library, I go remotely via a virtual private network on the Internet and, fortunately, I have access to that. I can also call the librarian who lets me in via the back door.
Michael: So for me, in one case, you are very free, and, in the other case, somewhat not free at all. I really do not know how to express that in any other way.
Olhoeft: I see what you are trying to say, but I would be less free without the device because it dramatically improves my functionality and quality of life, but also limits where I can go.
References
1. H. Burri and D. Senouf, “Remote monitoring and follow-up of pacemakers and implantable cardioverter defibrillators,” Europace, vol. 11, no. 6, pp. 701–709, 2009.
2. Staff. How can we help? Medtronic. [Online]. Available: http://professional.medtronic.com/customer-support/contact-us/index.htm#.Wbua5dWCzIU
3. A. Nordrum. ( 2016, Aug. 16 ). Popular Internet of Things forecast of 50 billion devices by 2020 is outdated. IEEE Spectrum. [Online]. Available: https://spectrum.ieee.org/tech-talk/telecom/internet/popular-internet-of-things-forecast-of-50-billion-devices-by-2020-is-outdated
4. G. Hernandez, O. Arias, D. Buentello, and Y. Jin. ( 2014 ). Smart Nest thermostat: A smart spy in your home. Blackhat. [Online]. Available: https://www.blackhat.com/docs/us-14/materials/us-14-Jin-Smart-Nest-Thermostat-A-Smart-Spy-In-Your-Home-WP.pdf
5. A. Greenberg. ( 2015, July 21 ). Hackers remotely kill a Jeep on the highway—with me in it. Wired. [Online]. Available: https://www.wired.com/2015/07/hackers-remotely-kill-jeep-highway/
6. M. Waibel. ( 2011, Feb. 17 ). BrainDriver: A mind controlled car. IEEE Spectrum. [Online]. Available: https://spectrum.ieee.org/automaton/transportation/human-factors/braindriver-a-mind-controlled-car
Authors
University of Wollongong, Australia
Katina Michael (katina@uow.edu.au) is a professor at the University of Wollongong, Australia, who has been researching the social implications of implantable devices for the last 20 years.
Citation: K. Michael, "Brain Pacemakers in Consumer Medical Electronics Improve Quality of Life-Part II: The Need for Patient Feedback in the Product Lifecycle Management," in IEEE Consumer Electronics Magazine, vol. 7, no. 6, pp. 51-54, Nov. 2018, doi: 10.1109/MCE.2018.2835879.